
Prostate adenoma (BPH)

The prostate is a gland located below the bladder through which the urinary tract (urethra) passes.
The central part of this gland increases in size with age: it is Benign Prostate Hypertrophy or prostate adenoma.
The most common symptoms are: difficulty urinating, delayed drops, difficulty initiating urination, frequent urination, urge to pee and get up several times at night.
The assessment includes an examination by the urologist. ECBU, creatinine testing, and urinary tract ultrasound are often requested.
PSA testing may be requested in patients who are candidates for prostate cancer screening.
MEDICAL TREATMENT

When symptoms impact quality of life, treatment can / should be offered.
There are several drug treatments with different modes of action.
These treatments will be taken over the long term and readjusted by your urologist according to the evolution of symptoms.
When medical treatment is no longer sufficient or if urinary problems become more complicated (urine retention, kidney failure, infections, bladder stones, etc.) surgical treatment which consists of unblocking the prostate should be considered. This procedure is not a total prostatectomy (removal of the entire gland for cancer) and does not have the same risks of consequences on urinary continence and does not cause erectile dysfunction.
ENDOSCOPIC ENUCLEATION OF THE PROSTATE: The revolution!

In this last ten years, endoscopic enucleation of the prostate has established itself as the new "Gold standard" for the treatment of benign prostatic hypertrophy.
The adenoma is no longer "planed" but completely enucleated like a walnut.
This technique has the advantage of combining the long-term efficacy of open surgery and the minimally invasive nature of endoscopic surgery.
The large prostate volume is no longer a constraint and even prostates weighing more than 200 g are operated on by natural means without scars with the patient leaving the day after the operation!
Since 2016, this technique has arrived in some Tunisian centers.
Classic techniques

Enucleation vs endoscopic resection of the prostate (a planing of the prostate): Prostate resection has historically been the benchmark against which all surgical procedures for the treatment of an enlarged prostate compare. Enucleation is promised to replace resection as the standard on the basis of several scientific publications demonstrating its equivalent if not superior results, and its lower percentage of postoperative complications. In addition, less than 1% of patients operated on by enucleation required reoperation for adenomatous regrowth within 8 years compared to a rate of 18% for reoperation with conventional resection.

Enucleation vs Open adenomectomy : Traditionally, men with a large prostate are offered open surgery: an adenomectomy. This is surgery that is associated with a high blood transfusion rate, prolonged bladder probing time, and hospital stays varying from 5 to 10 days. Unlike resection, endoscopic enucleation is a technique independent of the size of the adenoma. Therefore, enucleation is made to supplant open surgery for the treatment of large prostates.
In trained hands, this new technique makes it possible to operate on adenomas larger than 200 g.
Plasma vaporization

Prostate plasma vaporization is a recent technique that we also use in our clinic. It is indicated in elderly, so-called fragile patients and / or patients in whom anticoagulant treatment cannot be stopped. This technique allows excellent control of intra and postoperative bleeding. Several patients with indwelling bladder catheters, deemed inoperable by other techniques, were able to benefit from this new technique.
Green-light laser

Green-light laser photo-vaporization is a technique that uses the KTP laser (green laser). It is often indicated in very elderly patients and / or in patients on anti-coagulant therapy. Often indicated for small or medium volume prostates, this technique has a relatively high cost.

This consists of injecting micro-beads (or micro-particles) into the prostate arteries in order to obliterate them and therefore, theoretically, reduce the volume of the gland. The advantage of this technique is that it is done under local anesthesia, passing through the femoral (or radial) artery, but also that it preserves ejaculation. However, it requires continuous monitoring during the X-ray procedure. It therefore requires a high level of expertise and must be done in a specialized center to reduce the irradiation time (a few hours).
We do not have enough hindsight to judge the effectiveness of this new technique, but it seems that it lies between medical treatment and surgery (comparative studies are in progress). The improvement in symptoms seems to be significant in the case of a large prostate (> 80gr).
This technique is available in Tunisia.
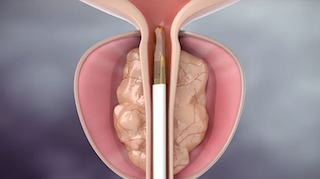
It is a recent, minimally invasive technique that uses pressurized water vapor to directly ablate (destroy) enlarged prostate tissue.
The doctor will use a camera that passes through the urethra to reach the prostate. A tiny amount of steam is injected into the swollen prostate tissue. The energy carried by the steam damages too many cells, causing them to die. Over time, the body absorbs the treated tissue, which retracts and symptoms are relieved.
It is a procedure that can be done under local anesthesia. The patient leaves the clinic the same day.
Improvement in symptoms begins to show 4-6 weeks after the procedure.
The great advantage of this technique is the complete preservation of sexuality and in particular of ejaculation.
According to the latest clinical studies, the efficacy is maintained for at least 5 years.
This technique is soon available in our center.
Cabinet d'urologie
Dr Wassim Chaabane
Centre Médical Coral
Centre Urbain Nord, 1082 Tunis
كورال الطبي
المركز العمراني الشمالي تونس
+216 71 947 574

Traitements innovants
Enucleation Prostatique au plasma
Laser pour calcul
micro-TESE
Varicocèle
Contact
Téléconsultation
A Propos
